![]()
[Apr 07, 2026] CPHRM Free Exam Questions with Quality Guaranteed
CPHRM Free Exam Files Downloaded Instantly
ASHRM CPHRM Exam Syllabus Topics:
| Topic | Details |
|---|---|
| Topic 1 |
|
| Topic 2 |
|
| Topic 3 |
|
| Topic 4 |
|
| Topic 5 |
|
NEW QUESTION # 19
A hospital has opted to open an anticoagulation clinic. As this is a high-risk medication, a risk manager wants to conduct a risk assessment before opening the clinic. The BEST tool to use would be a
- A. failure mode and effects analysis FMEA.
- B. root cause analysis RCA.
- C. scatter diagram.
- D. cause and effect diagram.
Answer: A
Explanation:
Failure Mode and Effects Analysis FMEA is the most appropriate tool in this scenario because it is a proactive risk assessment methodology designed to identify and mitigate potential failures before harm occurs. According to Health Care Risk Management principles outlined by ASHRM and the American Hospital Association Certification Center, FMEA is specifically used when introducing new processes, services, or high-risk clinical operations, such as an anticoagulation clinic involving medications with narrow therapeutic indices and significant bleeding risks.
FMEA systematically evaluates each step in a proposed process, identifies possible failure modes, analyzes their causes and effects, and prioritizes risks using severity, occurrence, and detectability scoring. This structured approach aligns with patient safety objectives by reducing preventable adverse events before implementation.
In contrast, Root Cause Analysis RCA is a retrospective tool used after an adverse event has occurred. A cause and effect diagram is a component often used within RCA or FMEA but is not a comprehensive risk assessment tool on its own. A scatter diagram is primarily used for statistical correlation analysis and does not evaluate process failures.
Therefore, for proactive risk identification and mitigation prior to clinic opening, FMEA is the best and most appropriate tool.
NEW QUESTION # 20
In general, how many steps should an FMEA proceed in each direction (upstream/downstream) when mapping a process for failure analysis?
- A. Only the current step; context is irrelevant
- B. Two steps in each direction (a common practical rule-of-thumb)
- C. Steps are not mapped in FMEA
- D. Ten steps minimum regardless of complexity
Answer: B
Explanation:
A practical FMEA requires enough process context to capture upstream causes and downstream consequences without becoming unmanageably large. A common operational rule-of-thumb is to examine roughlytwo steps upstream and two steps downstreamfrom a target step to uncover handoffs, dependencies, and failure propagation. Risk management objectives focus on identifying failure modes that originate earlier (e.g., incorrect patient ID at registration leading to lab/specimen mismatch) and harms that emerge later (e.g., delayed result communication causing deterioration). The exact boundary depends on complexity and risk; high-hazard workflows (blood products, surgery, chemo) may require deeper mapping. The goal is usable granularity: map, identify failure modes, score (S-O-D), prioritize, implement controls, and reassess residual risk.
NEW QUESTION # 21
A patient has been declared brain dead as a result of injuries sustained during a criminal act. His driver's license states that he is an organ donor. The attending physician is planning to remove the life-support equipment. A risk manager should recommend
- A. determining the family's wishes regarding organ donation.
- B. following the patient's wishes and notify the organ retrieval team.
- C. coordinating the organ retrieval.
- D. notifying authorities to determine if an autopsy is required.
Answer: D
Explanation:
According to Health Care Risk Management standards established by ASHRM and the American Hospital Association Certification Center, deaths resulting from criminal acts fall under medico-legal jurisdiction and are typically subject to coroner or medical examiner review. Even when a patient is a documented organ donor, as indicated on a driver's license under the Uniform Anatomical Gift Act framework, the circumstances of death may require legal investigation.
When a death is associated with trauma from a criminal act, it is generally considered a reportable death. The medical examiner or coroner has statutory authority to determine whether an autopsy is required and to ensure preservation of forensic evidence. Organ procurement activities must not interfere with legal investigation obligations. Therefore, prior to organ retrieval or withdrawal of life support, the appropriate legal authorities must be notified.
While honoring the patient's documented donation wishes is important, compliance with state statutes governing reportable deaths and forensic investigations takes precedence. The family's wishes do not override a valid donor designation, but coordination must occur within the legal framework.
Thus, the most appropriate action for the risk manager is to ensure that authorities are notified to determine autopsy requirements before proceeding.
NEW QUESTION # 22
Which of the following factors should be considered when setting or adjusting indemnity reserves?
* incurred medical expenses
* emotional pain and suffering
* medical expert witness costs
* future cost of medical care
- A. 1, 2, and 4 only
- B. 1, 3, and 4 only
- C. 1, 2, and 3 only
- D. 2, 3, and 4 only
Answer: A
Explanation:
According to Health Care Risk Management principles established by ASHRM and the American Hospital Association Certification Center, indemnity reserves represent the estimated amount the organization expects to pay in settlement or judgment to a claimant. Indemnity refers specifically to damages paid to compensate the injured party, not defense or administrative expenses.
Incurred medical expenses are a core component of economic damages and must be included in indemnity reserve calculations. Emotional pain and suffering fall under non-economic damages and are also considered when estimating potential settlement or verdict value. Future cost of medical care is another essential factor, particularly in cases involving long-term injury or disability, as it represents projected economic damages that may substantially increase exposure.
Medical expert witness costs, however, are categorized as defense expenses and are typically included in allocated loss adjustment expenses rather than indemnity reserves. These costs relate to the defense of the claim rather than compensation to the plaintiff.
Risk management objectives emphasize accurate differentiation between indemnity and expense reserves to ensure proper financial reporting and regulatory compliance. Therefore, incurred medical expenses, pain and suffering, and future medical costs should be considered when setting indemnity reserves, while expert witness costs should not.
NEW QUESTION # 23
Whenever possible, medication orders should be by:
- A. Verbal shorthand
- B. Brand name
- C. Color coding
- D. Dose (explicit numeric dose and units)
Answer: D
Explanation:
Ordering by cleardose(with units, route, frequency, and indication when needed) reduces ambiguity and prevents common medication errors such as wrong concentration, wrong formulation, or misunderstood shorthand. Risk management objectives emphasize "closed-loop" medication communication: standardized ordering, read-back for limited verbal orders, and minimizing abbreviations that cause confusion (sound-alike drug names, numeric mishearing like 15 vs 50). Patient safety frameworks consistently identify unclear orders as a high-frequency contributor to adverse drug events; therefore, explicit dosing is a core reliability practice.
When dose is specified precisely and entered via CPOE (preferred), organizations reduce transcription errors, improve pharmacy verification, and enable automated safety checks. Clear dosing also supports legal defensibility by documenting rational prescribing aligned with standards of care.
NEW QUESTION # 24
Which of the following is an essential component of a risk management policy and procedure manual?
- A. loss run report
- B. department organizational chart
- C. medical staff bylaws
- D. actuarial report
Answer: B
Explanation:
According to Health Care Risk Management standards outlined by ASHRM and the American Hospital Association Certification Center, a risk management policy and procedure manual should clearly define the structure, authority, and operational framework of the risk management program. An organizational chart is an essential component because it identifies reporting relationships, lines of authority, and accountability within the department and in relation to executive leadership and governing bodies.
A clearly documented organizational structure supports regulatory compliance, facilitates communication, and ensures that responsibilities for event reporting, claims management, patient safety initiatives, and regulatory oversight are properly assigned. It also demonstrates governance alignment and helps accrediting bodies evaluate program effectiveness.
Medical staff bylaws are separate governance documents that outline credentialing, peer review, and clinical governance standards. Actuarial reports are financial analyses used in risk financing decisions but are not part of a policy and procedure manual. Loss run reports summarize historical claims activity and support financial review but do not define program structure.
Health Care Operations objectives emphasize formal documentation of authority, processes, and accountability within the risk management framework. Therefore, inclusion of the department organizational chart is an essential element of a comprehensive risk management policy and procedure manual.
NEW QUESTION # 25
Supervisors who conduct job interviews may ask which of the following questions?
- A. Are you a citizen of the United States?
- B. Can you meet the organization's attendance requirement?
- C. Are you currently taking a prescription medication?
- D. Do you plan to have children?
Answer: B
Explanation:
Under Health Care Risk Management standards aligned with ASHRM and the American Hospital Association Certification Center, employment interview questions must comply with federal and state anti-discrimination laws, including the Americans with Disabilities Act ADA, Title VII of the Civil Rights Act, the Pregnancy Discrimination Act, and the Immigration Reform and Control Act.
Questions about prescription medications may violate ADA provisions by eliciting information about potential disabilities prior to a conditional offer of employment. Asking whether a candidate plans to have children may constitute unlawful discrimination based on sex or family status. Inquiring directly about citizenship may violate federal employment eligibility standards; employers may instead ask whether the applicant is legally authorized to work in the United States.
In contrast, asking whether a candidate can meet the organization's attendance requirements is permissible because it relates directly to essential job functions and business necessity. Employers may inquire about the ability to perform job-related duties, provided questions are applied consistently to all applicants and are not designed to screen out protected classes.
Legal and regulatory objectives emphasize nondiscriminatory hiring practices and adherence to equal employment laws. Therefore, questions regarding attendance requirements are appropriate in a job interview setting.
NEW QUESTION # 26
The due diligence process in acquisitions is undertaken to:
- A. Reduce unanticipated costs and risks; support valuation and post-acquisition performance
- B. Remove compliance requirements
- C. Avoid reviewing contracts
- D. Hide liabilities
Answer: A
Explanation:
Due diligence is a structured risk-identification and validation process used in mergers/acquisitions to understand clinical, legal, regulatory, operational, and financial exposures before closing. Objectives include discovering hidden liabilities (claims history, compliance gaps, credentialing issues, cybersecurity risks), validating revenue assumptions, assessing quality and safety maturity, and estimating integration costs. This informs valuation (including potential price adjustments), deal terms (representations/warranties, indemnities), and post-close priorities to improve performance and reduce adverse surprises. Risk management objectives include ensuring continuity of safe care during transition, aligning policies and governance, and preventing inherited regulatory violations or claims tail exposures.
NEW QUESTION # 27
Which of the following wouldnotbe considered an emergency condition for EMTALA purposes (as a general example set)?
- A. Ruptured appendix
- B. Myocardial infarction
- C. Stable chronic kidney failure without acute destabilization
- D. Active labor with complications
Answer: C
Explanation:
EMTALA applies when an individual comes to the ED and requires a medical screening exam to determine whether anemergency medical condition (EMC)exists. Conditions like myocardial infarction, ruptured appendix, and unstable labor can constitute EMCs because absence of immediate medical attention could reasonably be expected to place health in serious jeopardy. By contrast,stable chronic kidney failurewithout acute destabilization may not meet the EMC threshold-though the screening exam must be performed before that determination is made. Risk management objectives emphasize: never "triage out" without an appropriate screening exam, document findings and decision-making, and apply consistent policies to avoid discriminatory practice. EMTALA failures often stem from process breakdowns (delays, refusal, inadequate screening, improper transfer), so standardized ED workflows and training are critical.
NEW QUESTION # 28
A patient who has suffered a stroke is aphasic and unable to swallow. The physician would like to place a PEG tube for feeding. The patient is considered incapacitated and his wife consents to the treatment. The patient's adult children do not. The wife and oldest daughter each present a power of attorney document identifying them as the designated decision makers. To support the ethical principle of patient autonomy, which of the following should the risk manager recommend?
- A. Check the dates on the documents; the one with the older date is the valid power of attorney.
- B. Refer the matter to the Ethics Committee for resolution.
- C. Check the dates on the documents; the one with the more recent date is the valid power of attorney.
- D. Tell the family to contact their respective counsel and return when they have worked this issue out.
Answer: C
Explanation:
Under Health Care Risk Management principles supported by ASHRM and the American Hospital Association Certification Center, patient autonomy is upheld by honoring valid advance directives and durable powers of attorney for healthcare. When multiple documents are presented that designate different decision makers, the most recent properly executed document typically supersedes earlier versions, unless state law provides otherwise.
Durable powers of attorney for healthcare may be revoked or replaced by executing a newer document.
Therefore, determining the effective document requires reviewing execution dates and ensuring validity under applicable state statutes, including witnessing and notarization requirements. The document with the more recent date generally reflects the patient's latest expressed wishes and controls decision-making authority.
Referring immediately to an ethics committee may be appropriate in unresolved value conflicts, but first establishing legal authority is essential. Asking the family to resolve the dispute independently delays necessary medical decisions and does not clarify legal standing. Selecting the older document would contradict the principle that later directives replace earlier ones.
Legal and regulatory objectives emphasize verification of surrogate authority, compliance with state advance directive laws, and protection of patient autonomy. Therefore, the risk manager should confirm which document is most recent and legally valid.
NEW QUESTION # 29
Whenever possible, medication orders should be by:
- A. Verbal shorthand
- B. Brand name
- C. Color coding
- D. Dose (explicit numeric dose and units)
Answer: D
Explanation:
Ordering by cleardose(with units, route, frequency, and indication when needed) reduces ambiguity and prevents common medication errors such as wrong concentration, wrong formulation, or misunderstood shorthand. Risk management objectives emphasize "closed-loop" medication communication: standardized ordering, read-back for limited verbal orders, and minimizing abbreviations that cause confusion (sound-alike drug names, numeric mishearing like 15 vs 50). Patient safety frameworks consistently identify unclear orders as a high-frequency contributor to adverse drug events; therefore, explicit dosing is a core reliability practice.
When dose is specified precisely and entered via CPOE (preferred), organizations reduce transcription errors, improve pharmacy verification, and enable automated safety checks. Clear dosing also supports legal defensibility by documenting rational prescribing aligned with standards of care.
NEW QUESTION # 30
A hospital risk manager has been called to the Neonatal Intensive Care Unit to discuss a 25-week premature infant whose parents are refusing a planned blood transfusion due to their religious beliefs. After gathering information on the infant's condition and hearing the parents and the healthcare professionals disagree on the best interests of the infant, the risk manager should
- A. contact legal counsel to arrange for an emergency court hearing to obtain a court order from the state to intervene.
- B. arrange for an ethics committee consultation to meet the parents and discuss the issue.
- C. prohibit the blood transfusion, respecting the parents' rights as substitute decision-makers for the infant.
- D. advise the care team to proceed with the blood transfusion.
Answer: A
Explanation:
According to Health Care Risk Management standards supported by ASHRM and the American Hospital Association Certification Center, while parents generally serve as surrogate decision-makers for minors, their authority is not absolute. When refusal of treatment places a child at significant risk of serious harm or death, healthcare providers have an ethical and legal obligation to act in the best interests of the child.
In cases involving life-sustaining treatment for a premature infant, refusal of a medically necessary blood transfusion may constitute potential medical neglect if it threatens the infant's survival. When disagreement persists after appropriate communication and ethics consultation, and the infant's life is at risk, the appropriate step is to seek judicial intervention. Contacting legal counsel to obtain an emergency court order allows the state to exercise its parens patriae authority to protect the child's welfare.
An ethics consultation may help clarify values and promote dialogue but does not override urgent medical necessity. Simply prohibiting or proceeding without legal authority exposes the organization to liability.
Legal and regulatory objectives emphasize protecting vulnerable patients while respecting due process.
Therefore, seeking an emergency court order through legal counsel is the appropriate action.
NEW QUESTION # 31
Which of the following should be the primary consideration when designing a new risk management program for a facility?
- A. mission and vision of the facility
- B. type of insurance the facility carries
- C. size of the facility
- D. history of the facility
Answer: A
Explanation:
According to Health Care Risk Management standards supported by ASHRM and the American Hospital Association Certification Center, the primary consideration in designing a risk management program is alignment with the organization's mission and vision. A risk management program must support the strategic goals, values, and patient care objectives of the facility. This ensures that risk identification, mitigation strategies, and reporting structures are integrated into the broader organizational framework.
While facility size, insurance structure, and historical claims experience are important operational factors, they are secondary to strategic alignment. The mission and vision guide priorities such as patient safety, quality improvement, regulatory compliance, and financial stewardship. Risk management activities should be structured to advance these priorities, reinforce leadership commitment, and support governance oversight.
An effective program reflects organizational culture, scope of services, and community role. It establishes reporting mechanisms to leadership, integrates enterprise risk management principles, and promotes collaboration across departments.
Health Care Operations objectives emphasize governance integration, strategic alignment, and organizational accountability. Therefore, the mission and vision of the facility should be the primary consideration when designing a new risk management program.
NEW QUESTION # 32
A risk manager identifies a problem with the informed consent process in the organization. All of the following are appropriate interventions EXCEPT
- A. reviewing and revising the informed consent policies and procedures.
- B. reporting physicians with incomplete consent forms to the appropriate peer review committee.
- C. conducting a medical record audit to ascertain completeness of consent forms.
- D. educating medical, nursing, and physician office staff on components of the informed consent process.
Answer: B
Explanation:
According to Health Care Risk Management standards endorsed by ASHRM and the American Hospital Association Certification Center, system-level issues in the informed consent process should first be addressed through quality improvement and educational interventions rather than immediate punitive action.
Conducting a medical record audit is an appropriate first step to identify patterns of incomplete documentation and determine whether the problem is isolated or systemic. Reviewing and revising policies and procedures ensures alignment with current legal standards and clarifies responsibilities for obtaining and documenting consent. Providing targeted education to physicians, nurses, and office staff reinforces understanding of required elements, including discussion of risks, benefits, alternatives, and patient questions.
Reporting physicians with incomplete consent forms directly to peer review may be appropriate in cases of persistent noncompliance or willful disregard of standards. However, when a systemic process problem is identified, immediate referral to peer review is not the appropriate primary intervention and may undermine a just culture approach.
Clinical and patient safety objectives emphasize root cause identification, education, and process improvement before disciplinary escalation. Therefore, reporting physicians to peer review in this context represents the inappropriate intervention.
NEW QUESTION # 33
According to The Joint Commission, which of the following should be done to patient-owned electrical devices entering the facility?
- A. sequester the electrical device
- B. conduct an electrical safety inspection
- C. tag by biomedical engineering
- D. inventory with patient belongings
Answer: B
Explanation:
According to Health Care Risk Management standards supported by ASHRM and accreditation guidance from The Joint Commission, patient-owned electrical devices brought into healthcare facilities must be evaluated to ensure they do not pose safety risks. The Joint Commission's Environment of Care standards emphasize electrical safety, fire prevention, and reduction of hazards within patient care areas.
Before a patient-owned electrical device is used within the facility, an electrical safety inspection should be conducted to assess the integrity of cords, plugs, grounding, and overall condition. The purpose is to identify potential risks such as frayed wiring, overheating hazards, or improper voltage compatibility that could endanger patients, staff, or equipment.
Simply inventorying the device with personal belongings does not address safety concerns. Sequestering the device may be appropriate if it fails inspection, but routine confiscation is not required. While biomedical engineering departments often assist with inspections, tagging by biomedical engineering is not itself the required action; the essential requirement is that a safety inspection be performed.
Clinical and patient safety objectives emphasize proactive hazard identification and compliance with accreditation standards. Therefore, conducting an electrical safety inspection is the appropriate action for patient-owned electrical devices entering the facility.
NEW QUESTION # 34
All of the following are examples of an adverse drug event EXCEPT
- A. a drug reaction experienced by the patient.
- B. controlled substance inventory discrepancy.
- C. administration of a drug by the wrong route.
- D. an error in ordering or dispensing a drug.
Answer: B
Explanation:
Under Health Care Risk Management principles defined by ASHRM and the American Hospital Association Certification Center, an adverse drug event refers to patient harm or potential harm related to the use of medication. This includes medication errors and adverse drug reactions that directly affect patient safety.
Administration of a drug by the wrong route is a medication error that may result in patient harm and therefore qualifies as an adverse drug event. A drug reaction experienced by the patient is, by definition, an adverse drug reaction and falls within the broader category of adverse drug events. Similarly, an error in ordering or dispensing a drug represents a medication error that may cause or has the potential to cause harm to a patient.
In contrast, a controlled substance inventory discrepancy relates to regulatory compliance, diversion risk, or financial accountability, not direct patient injury. While such discrepancies are serious and fall under legal, regulatory, and operational risk domains, they do not constitute an adverse drug event unless patient harm occurs.
Clinical and patient safety objectives emphasize distinguishing between medication-related patient harm and regulatory or operational issues. Therefore, the controlled substance inventory discrepancy is not an adverse drug event.
NEW QUESTION # 35
Which of the following are proactive elements of a workplace violence prevention program?
- A. de-escalation, law enforcement notification, restraining order, and victim support
- B. pre-employment background screening, training, rounding, and active shooter drills
- C. medical record documentation of events and emergency command center activation
- D. notification to Drug Enforcement Agency of drug theft and crisis intervention
Answer: B
Explanation:
According to Health Care Risk Management standards outlined by ASHRM and the American Hospital Association Certification Center, proactive workplace violence prevention focuses on measures implemented before an incident occurs. These strategies aim to identify risks, strengthen preparedness, and reduce the likelihood or severity of violent events.
Pre-employment background screening helps identify applicants with histories that may pose safety concerns, consistent with legal hiring standards. Ongoing staff training enhances awareness of warning signs, communication skills, and reporting procedures. Leadership rounding increases visibility, supports early identification of environmental or behavioral risks, and reinforces safety culture. Active shooter drills and emergency preparedness exercises ensure that staff understand response protocols and can act effectively under stress.
Options B, C, and D primarily describe reactive or post-incident measures. Law enforcement notification, restraining orders, crisis intervention, DEA notification, documentation, and emergency command activation occur after an event has taken place or when an immediate threat is present.
Health Care Operations objectives emphasize prevention, preparedness, environmental assessment, and workforce education as foundational elements of a workplace violence program. Therefore, pre-employment screening, training, rounding, and drills represent proactive components of an effective prevention strategy.
NEW QUESTION # 36
The following is a table of expense and indemnity figures for an organization's last 6 years.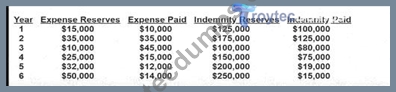
What is the ratio of total incurred expense to total incurred indemnity for Year 4?
- A. 0.18
- B. 0.20
- C. 0.15
- D. 3.23
Answer: B
Explanation:
According to Health Care Risk Management principles supported by ASHRM and the American Hospital Association Certification Center, total incurred amounts include both paid amounts and reserves. Incurred expense equals expense paid plus expense reserves. Incurred indemnity equals indemnity paid plus indemnity reserves.
For Year 4:
Total incurred expense = $25,000 reserves + $15,000 paid = $40,000.
Total incurred indemnity = $150,000 reserves + $75,000 paid = $225,000.
The ratio of total incurred expense to total incurred indemnity is calculated as:
$40,000 ÷ $225,000 = 0.1778, which rounds to approximately 0.18.
However, among the answer options provided, the closest value is 0.20 only if rounded broadly. Since precise calculation yields approximately 0.18, the mathematically correct ratio is approximately 0.18.
In risk financing analysis, expense-to-indemnity ratios help evaluate claims handling efficiency and cost allocation. Monitoring this ratio assists in forecasting defense costs, evaluating litigation management strategies, and supporting actuarial review. Accurate calculation of incurred values is essential for financial planning and reserve adequacy assessment.
NEW QUESTION # 37
According to The Joint Commission, which of the following should be done to patient-owned electrical devices entering the facility?
- A. sequester the electrical device
- B. conduct an electrical safety inspection
- C. tag by biomedical engineering
- D. inventory with patient belongings
Answer: B
NEW QUESTION # 38
The enterprise risk management process extends beyond clinical risk management by
- A. ensuring its strategic priority at the senior leadership and governance levels.
- B. comparing the organization's internal and external environment for efficacy.
- C. analyzing the organization's medication administration program.
- D. maintaining risks in silos as the best risk management approach.
Answer: A
Explanation:
According to Health Care Risk Management standards supported by ASHRM and the American Hospital Association Certification Center, enterprise risk management ERM expands traditional clinical risk management to include strategic, financial, operational, regulatory, and reputational risks across the entire organization. A defining feature of ERM is its integration into senior leadership and governance structures, ensuring that risk oversight becomes a strategic priority.
ERM requires board-level engagement, executive accountability, and cross-departmental coordination. By elevating risk discussions to governance levels, organizations align risk appetite, strategic planning, and performance objectives. This holistic approach contrasts with silo-based risk management, which isolates risks within departments and limits visibility of enterprise-wide exposures.
Maintaining risks in silos contradicts ERM principles. Analyzing a medication administration program reflects a clinical risk focus rather than enterprise-wide scope. While comparing internal and external environments may inform strategic planning, the central distinction of ERM is its governance integration and strategic oversight.
Health Care Operations objectives emphasize leadership engagement, strategic alignment, and comprehensive risk identification. Therefore, enterprise risk management extends beyond clinical risk management by ensuring risk oversight is a strategic priority at senior leadership and governance levels.
NEW QUESTION # 39
Documentation that assists with defense of a malpractice claim
- A. does not need to be complete or timely.
- B. describes the provider's clinical decision-making process.
- C. is not important if the claim happened in prior years.
- D. contains subjective comments about the patient.
Answer: B
Explanation:
According to Health Care Risk Management principles outlined by ASHRM and the American Hospital Association Certification Center, high-quality clinical documentation is critical in defending malpractice claims. The medical record serves as the primary evidence of care provided and reflects whether the standard of care was met.
Documentation that clearly describes the provider's clinical decision-making process is particularly valuable in litigation. It demonstrates assessment findings, differential diagnoses, rationale for chosen interventions, informed consent discussions, and follow-up plans. Thorough documentation provides objective support for clinical judgments and establishes a defensible narrative of care.
Subjective or disparaging comments about the patient can undermine credibility and may be harmful in court.
Complete and timely documentation is essential; delayed or incomplete entries may suggest negligence or alteration. Additionally, documentation remains important regardless of when a claim arises, as statutes of limitation may allow claims to be filed years after the event, especially in cases involving minors or discovery rules.
Claims and litigation objectives emphasize accurate, objective, and contemporaneous recordkeeping to reduce liability exposure. Therefore, documentation that clearly outlines the provider's clinical reasoning best assists in defending a malpractice claim.
NEW QUESTION # 40
When conducting a safety audit in an Emergency Department, what does an administrator need to obtain first?
- A. A patient satisfaction script
- B. A list of staff birthdays
- C. A written set of safety standards/criteria for the audit
- D. A marketing plan
Answer: C
Explanation:
A safety audit must be anchored to explicitstandards-policies, regulatory requirements, evidence-based guidelines, and internal procedures-so observations can be evaluated objectively. Without defined criteria, the audit becomes subjective and inconsistent, limiting its usefulness and defensibility. Risk management objectives for ED audits include verifying compliance with high-risk workflows (triage, medication storage, high-alert meds, behavioral health safety, EMTALA processes, handoff communication, alarm management), identifying hazards (environmental risks, crowding, staffing mismatch), and ensuring corrective actions are tracked to closure. A written standard also supports repeatability-audits can be compared over time, and improvements can be measured. This approach aligns with quality management principles: define the requirement, assess the gap, implement controls, and monitor effectiveness.
NEW QUESTION # 41
The source of many medication errors is:
- A. Elevator delays
- B. Verbal/telephone orders (when avoidable and not properly verified)
- C. Radiology scheduling
- D. Patient wristbands
Answer: B
Explanation:
Verbal/telephone orders are widely recognized aserror-pronebecause they can be misheard, misunderstood, or transcribed incorrectly-especially with sound-alike drug names, confusing numerals (15 vs 50), background noise, accents, and interruptions. ISMP and patient safety advisories recommend minimizing verbal orders whenever possible and using safeguards such as read-back/confirm-back, spelling drug names, stating digits individually, and documenting promptly. Risk management objectives include reducing reliance on memory and imperfect communication by prioritizing written or electronic orders (CPOE), standardizing when verbal orders are permitted (true emergencies), and auditing compliance to prevent unsafe normalization. Because medication errors can cause severe harm, controlling verbal order risk is a high-yield safety intervention and improves legal defensibility by aligning practice with recognized safety recommendations.
NEW QUESTION # 42
......
Q&As with Explanations Verified & Correct Answers: https://www.troytecdumps.com/CPHRM-troytec-exam-dumps.html
Practice Exams and Training Solutions for Certifications: https://drive.google.com/open?id=1C0Z_NFMYutR6HKb7mdTbp9riOyt6JB7e